– by Wood Institute travel grantee Laura Smith*
On November 1, 1874, Dr. James H. Lenow procured the cadaver of an African American man from the state penitentiary in Arkansas and began dissecting it in a shed at the Little Rock Barracks, a military facility. Lenow would become an early faculty member at what would eventually be known as the University of Arkansas Medical School (UAMS) which was also located in Little Rock. The story of the dissection gave him prestige among the city’s residents and inspired local confidence in a growing medical status in the South. Lenow’s was the first legal dissection in Arkansas, and the state was so mesmerized by the deed that they built a monument to the dissection in May of 1927 on the spot it took place. The monument still stands today.

I have always found this story fascinating because it perfectly illustrates several aspects about the history of medicine and medical education. It shows that medicine for much of history was self-taught, just as Lenow took it upon himself to explore the body in dissection. More importantly, this dissection shows that the history of medical education is a story of two communities—first, the medical community that created universities and provided medical education, and second, the community who received the schools, the teaching, and the medical care. For those outside the university medical community, medicine and medical knowledge sometimes advanced at the expense of people who had the least political and economic power. One of the main purposes of medical schools—not to mention one of the key aspects of their survival—has always been their attempt to mediate tensions between the two communities and provide at least the appearance of benefit to the cities surrounding medical schools. My time at the Historical Medical Library was important for me primarily because it holds sources relating to attempts by medical schools to improve community standing but also manage competition between medical schools which eroded respect in the medical profession at large.
Most of the discourse on university obligations to their local town residents emerged in the 1800s, the same century as Lenow’s dissection. Thomas Duche Mitchell was a professor at the Transylvania University in Lexington, Kentucky prior to his arrival as a chair at the University of Pennsylvania Medical Department. He composed the pamphlet, The Reciprocal Obligations of Professors and Pupils: An Introductory Lecture in 1845, in which he pointed out the importance of the community as a whole in supporting the success of a medical school. He noted that the medical school is primarily a public institution: “An incorporated medical school is, in a certain and very important sense, public property. Its very existence, and above all, its success is dependent on public approbation and regard; not on the whims and caprices of the selfish, the conceited, and the arrogant, who are incompetent to judge of the merits of any public institution, but on the good sense of the well informed, the well-meaning, and the judicious portion of society”. Medical schools were a virtue of public service and success of communities according to Mitchell, but at the same time, communities often criticized medical men, and Mitchell defensively questions whether the public is worthy of understanding the nature of medicine.
One of the biggest obstacles to a medical school’s success were the rivalries between other local schools or doctors that contributed to an overall feeling among lay people that doctors had no consensus on medical ideas. Schools fought bitterly with each other; one example of these feuds that I explore in my dissertation is between medical schools in Lexington and Louisville, Kentucky. Dr. James Conquest Cross, a professor at the Medical Department of Transylvania University in Lexington, argued in his “Thoughts on the Policy of Establishing A School of Medicine in Louisville” that Louisville needed a medical school because Lexington’s was subpar. He said Transylvania gave no clinical experience and offered no opportunities for students to dissect cadavers. Whether or not it was true, his statements received much attention as the next few years mired the medical community in conflict through Cross’s expulsion from Transylvania and the subsequent pamphlets the doctors produced on whether or not it was just.
Though much of what I’ve discussed occurred in the 1800s, attempts to control existing negative perception of doctors and establish more successful and better respected medical universities began long before Lenow’s dissection. John Morgan’s A Discourse Upon the Institution of Medical Schools in America recommended that medical schools force their students to specialize. He argued for stronger regulation of physicians who he felt dabbled in too many aspects of medicine with little success. “Great is the havoc,” Morgan lamented, “which his ignorance spreads on every side, robbing the affectionate husband of his darling spouse, or rendering the tender wife a helpless widow, increasing the number of orphans”. Morgan was neither the first nor the last to argue that bad medical schools produced bad doctors, and bad doctors hurt the perception of the profession as a whole.
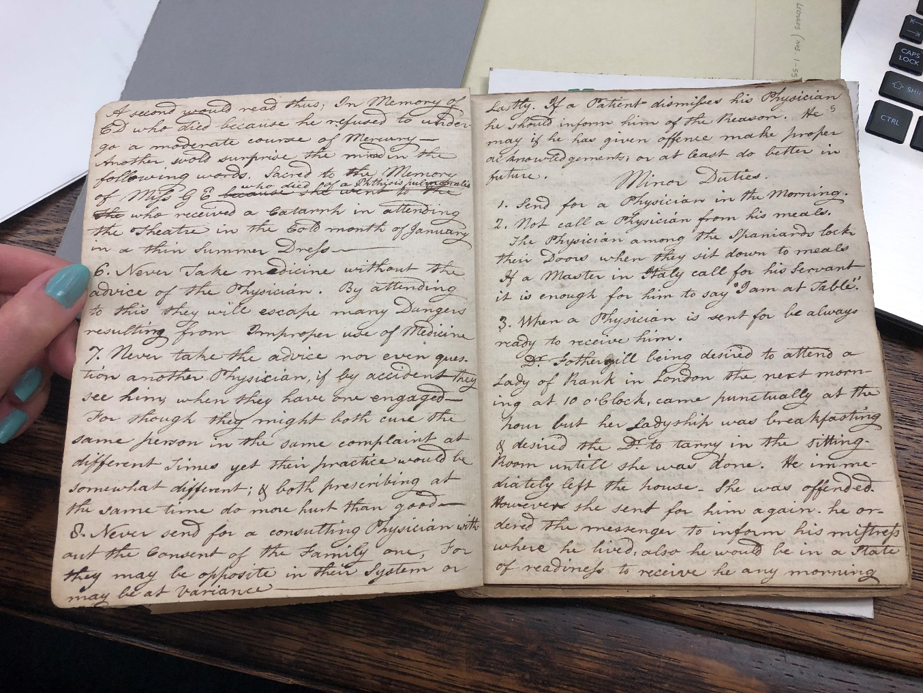
Benjamin Rush, one of Philadelphia’s most famous and prolific physicians, also discussed the importance of lay community respect for medical schools and doctors. One of the most helpful collections the Historical Medical Library provided was the Daniel J. Swinney Papers. Swinney was a student of Benjamin Rush, and Rush talked a lot about how to deal with patients receiving medical care. Rush began his lectures saying that patients had certain responsibilities to physicians which he listed out. Patients had the responsibility to choose physicians with proper education, follow what the physician said alone and not take medicine without his advice, and ultimately, be honest with his physician and never slander him. Physicians also had responsibilities to patients, such as going up the stairs before a lady to protect her modesty and letting the patient and family tell you what they think caused the sickness.
UAMS’ website today lists their mission statement and discusses why medical schools are important. “The mission of UAMS is to improve the health, health care and well-being of Arkansans and of others in the region, nation and the world by…providing high-quality, innovative, patient- and family–centered health care and specialty expertise not routinely available in community settings.” UAMS treats hundreds of thousands of patients in Arkansas and trains physicians for rural areas. Clearly, community interactions and relationships are high priorities for UAMS, but they have also been a concern for medical schools from much earlier days. We have to contextualize this relationship between the two communities, and I appreciate the efforts of the Historical Medical Library to protect and provide access to sources which document the history of medical education.
*Laura Smith is a Ph.D. Candidate at the University of Arkansas. She received an F.C. Wood Institute Travel Grant from the College of Physicians of Philadelphia in June 2019.