– by Kristen Pinkerton, Library Assistant
For the month of October, the theme the Historical Medical Library has chosen to highlight is skeletons. Skeletons are commonly viewed as creepy or associated with death and horror, particularly around Halloween. As a trained osteologist, however, I view them as a beautiful structure that supports the human form. This selected theme was an exciting chance for me to explore the fascinating materials we house regarding the human skeleton. While searching through our catalog I came across multiple monographs that piqued my interest.
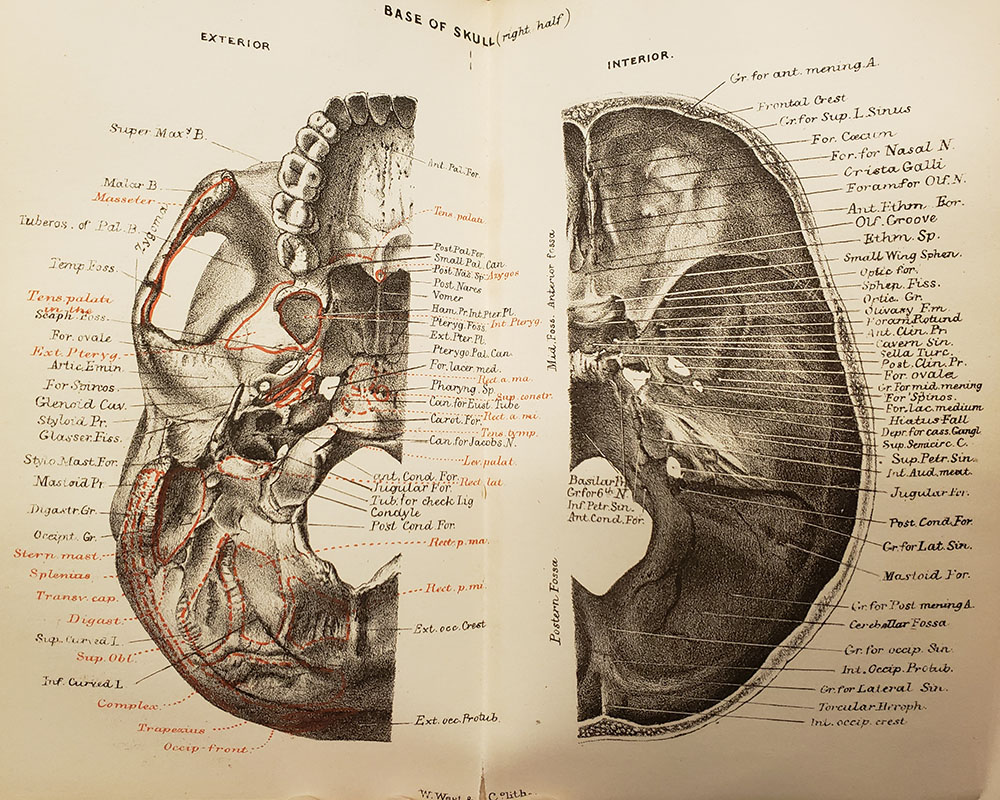
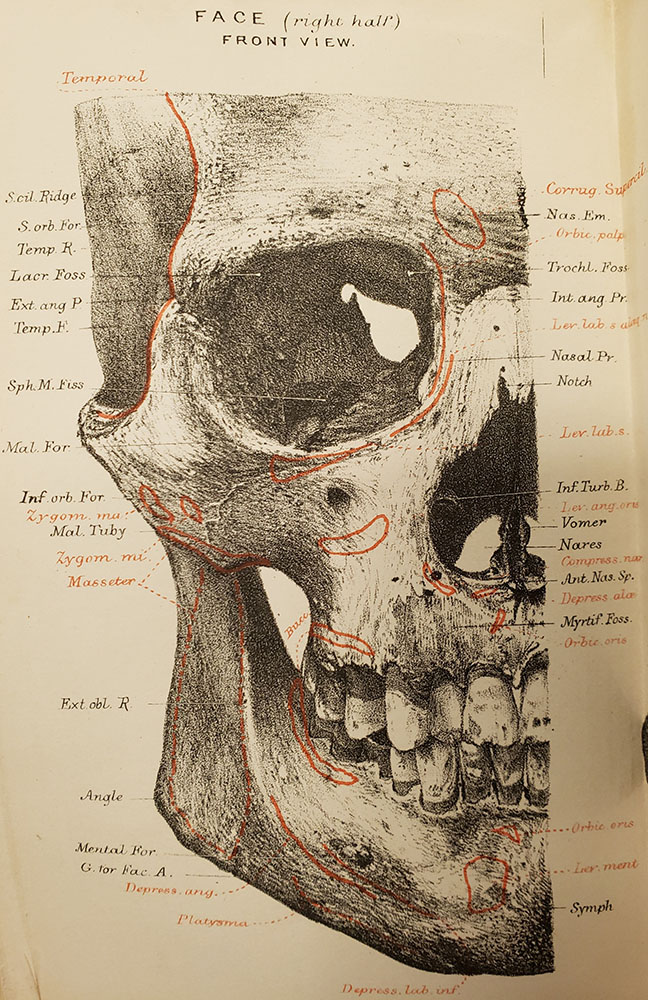
The first monograph I discovered was W.W. Wagstaffe’s The Student’s Guide to Human Osteology (1875). Wagstaffe begins by introducing the core purposes of the human skeleton which are essential to understanding the human body. Primarily, the human skeletal system is the supporting framework of our bodies and provides protection for our delicate organs. It also provides muscle attachments and levers for movement. Our muscles are the connective tissue that provide movement for our skeletons, while tendons attach muscle to bone and ligaments attach bone to bone. While our skeletons are influenced by genetics, other factors can play a role as well such as diet and activity. This means that no two skeletons are the same!
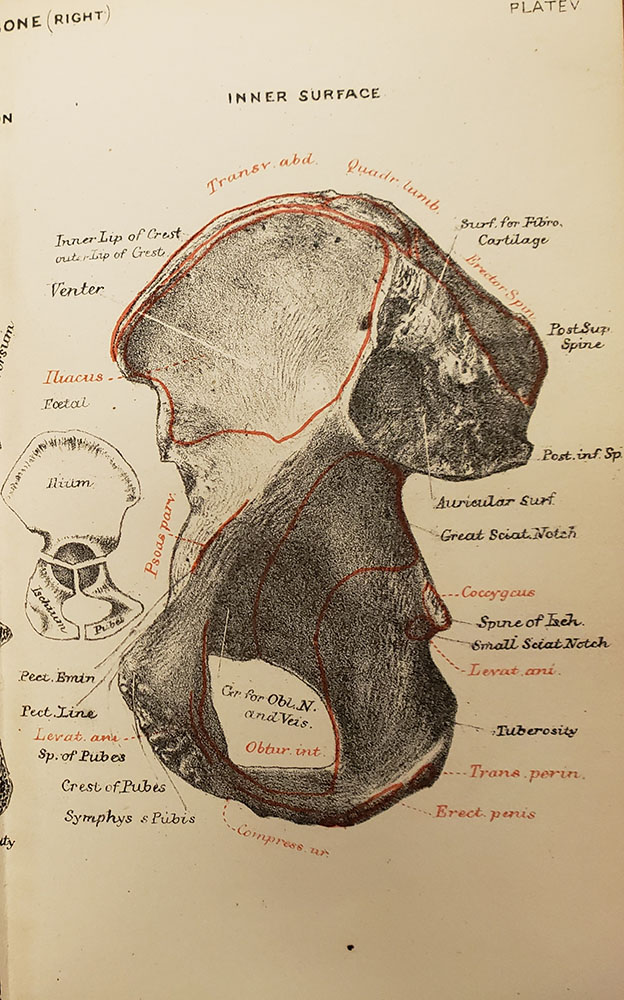
After laying out the main purposes of the skeleton, Wagstaffe’s monograph goes into detailed descriptions of each bone in the body. He also includes incredibly beautiful, detailed illustrations of each bone as well. Some of my personal favorites are the illustrations of the skull and the ossa coxae (innominate).
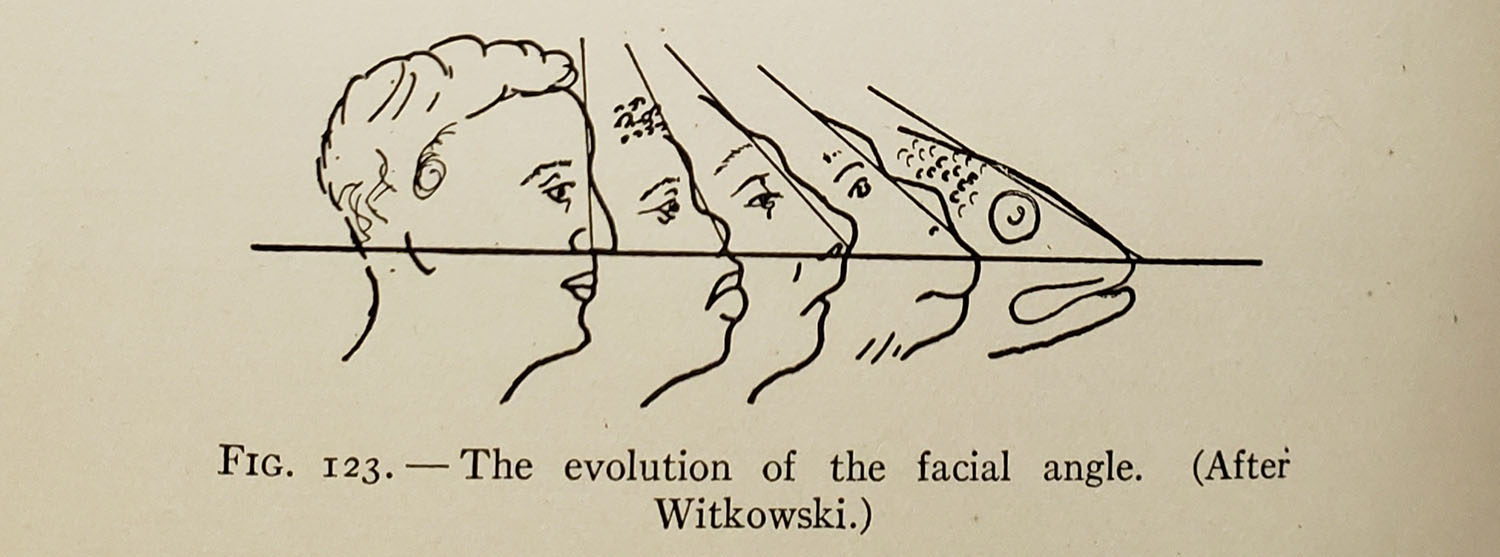
The next monograph I came across was The Human Skeleton: An Interpretation (1918) by Herbert Eugene Walter. Walter’s monograph discusses the structural evolution of the skeleton as a system of protection and scaffolding for the human body. He frames this idea with examples of the evolution of organisms and animals and compares them to humans. This resulted in some comparative illustrations that gave me a bit of a chuckle. One illustration comparing nose shapes uses five men and an elephant to showcase differences.

Another illustration meant to showcase the evolution of the angle of the face starts with a human face that morphs into a fish face.
After looking through materials on the foundation of the human skeletal system, I wanted to investigate what our collection may contain pertaining to skeletal trauma. My particular area of interest in graduate school was blunt force, sharp force, and gunshot trauma. Those are the three major classifications of skeletal trauma used by anthropologists. When it comes to discussing skeletal trauma, it is important to understand the basic composition of bone and how it reacts to outside forces. Bone consists of porous trabecular bone on the inner layer and denser cortical bone on the outer layer. Its composition of organic and inorganic material is what gives bone its elasticity and results in it being stronger in compression than tension. Bone is considered an anisotropic material, which means it can handle stress better in one direction. There are many variables that contribute to bone fracturing, such as direction, rate of loading, energy, and duration. Bone is able to withstand a greater load if it is applied at a slower rate, and responds as a brittle material when loaded with a high-speed force. Our bones have plasticity, which means they are able to be molded by force. Patterns of damage to the skeleton differ depending upon whether it is the long bones, such as the femur and humerus, or the flat bones, such as the ones that comprise the skull. I found a couple really fascinating monographs that focus on ballistic trauma from war time injuries while delving through our collection.
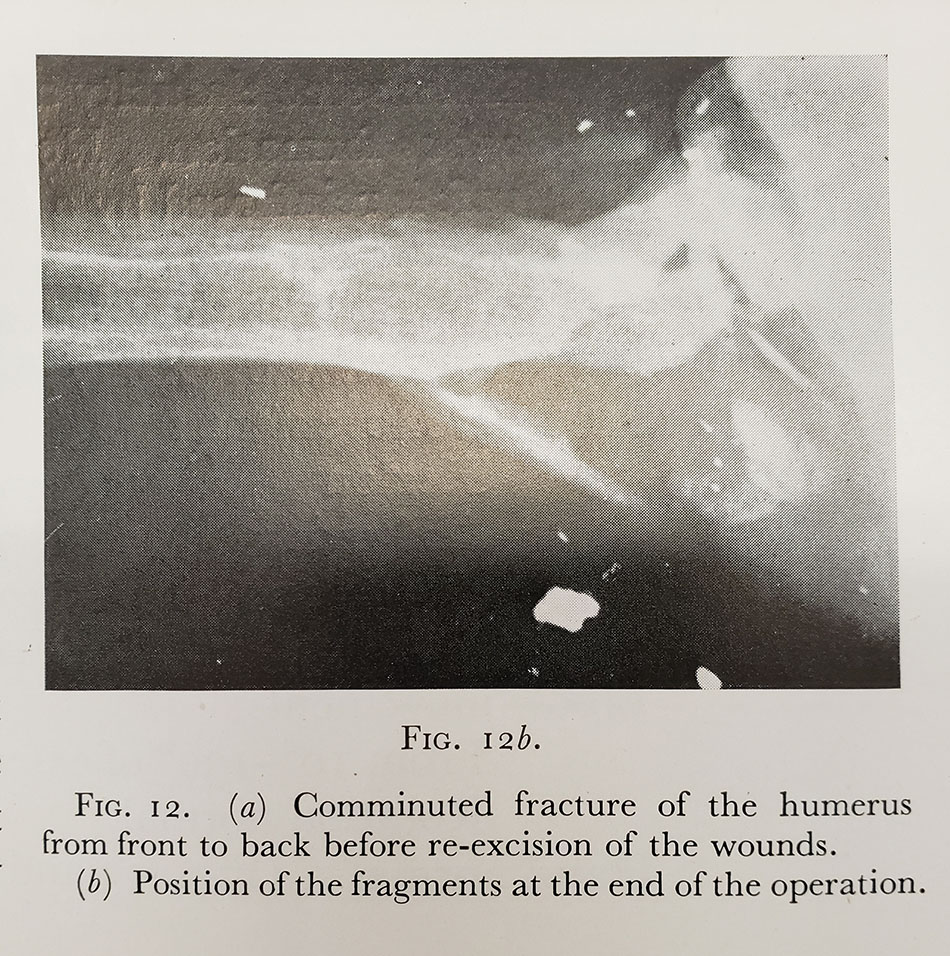
An Atlas of Traumatic Surgery Illustrated Histories of Wounds of the Extremities (1949) by Josep Truetta, M.D., is a fascinating case study of treatment of war time injuries through photography. Dr. Truetta was a surgeon at the Wingfield-Morris Orthopaedic Hospital in Oxford during WWII and recorded his treatment of the wounds with bullet point notes and photographs. Many of the wounds documented in his monograph are comminuted fractures of the long bones. Typical causes of the wounds Dr. Truetta treated were bullets and mortar bombs. A fracture is classified as comminuted when the bone breaks into more than two parts and is typically the result of blunt force and gunshot trauma.
While searching through our collection I wanted to find materials that better illustrate trauma patterns on bone. This search led me to the monograph Gunshot Injuries: How they are inflicted, their complications and treatment (1916) by Colonel Louis A. La Garde, which delves into gunshot wounds military surgeons would typically encounter. He explains the different military projectiles, explosives, and firearms, and the type of wounds these cause in specific parts of the body. He also explains typical treatment for these injuries. Most of his work is focused on the Civil War. My favorite images included in his monograph are the ones showcasing gunshot trauma on the bones. For those who are not in the medical profession, it may be easier to see the impact of trauma on bone when looking at it directly rather than an X-ray.
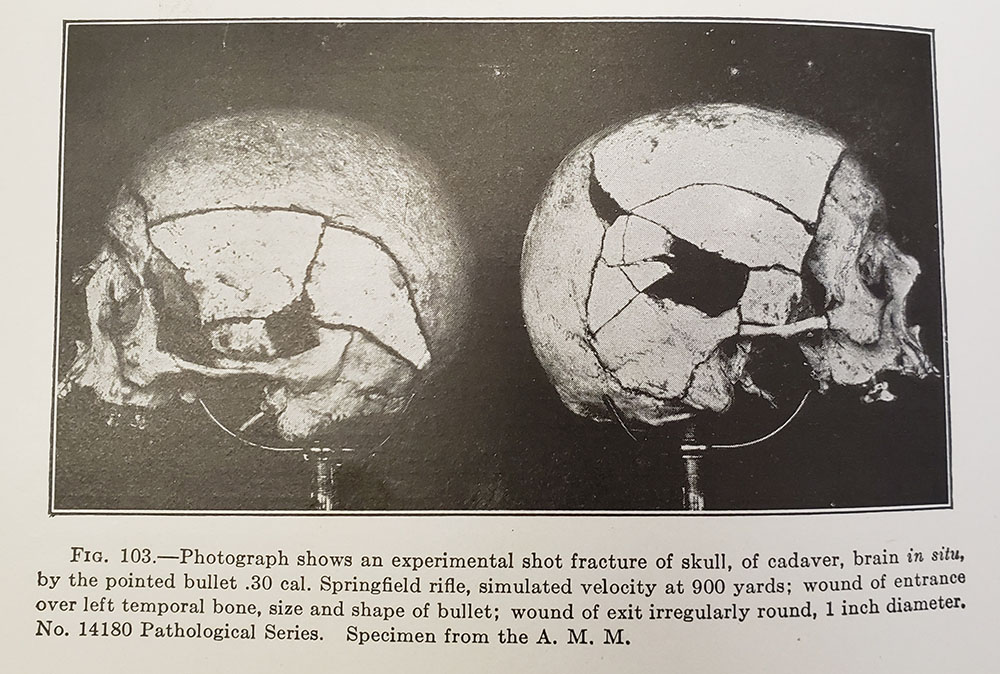
As can be seen in the above image, gunshot entrance wound fractures in the skull are typically circular in shape and can have a punched out appearance, while exit wounds are typically larger and irregular in shape. Radiating and concentric fractures from the impact of the bullet can also be seen in the image. Radiating fractures travel away from the entrance wound, while concentric fractures form perpendicular to them. An incredible fact is that radiating fractures travel across the skull faster than the bullet exits. This can help experts determine the entrance versus exit wound, as fracture lines will be arrested by pre-existing lines, which is known as Puppe’s Rule.
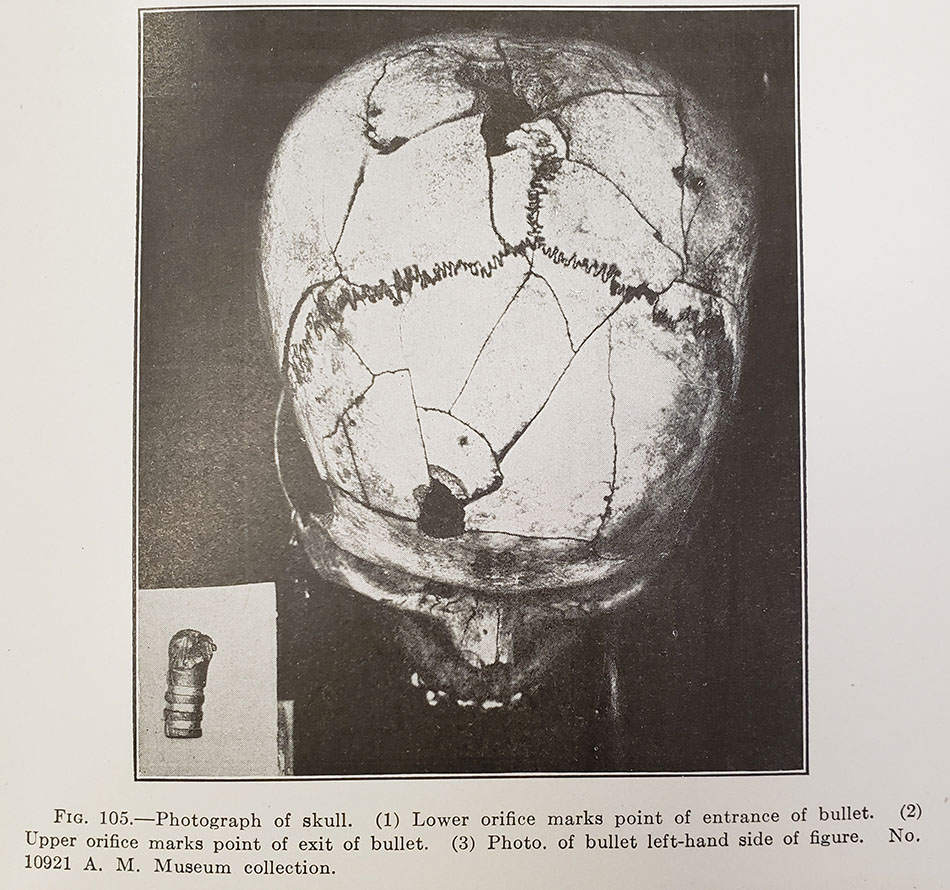
In the above image we can again see the presence of an entrance and exit wound with radiating and concentric fractures. The entrance wound is much a cleaner hole than the exit wound.
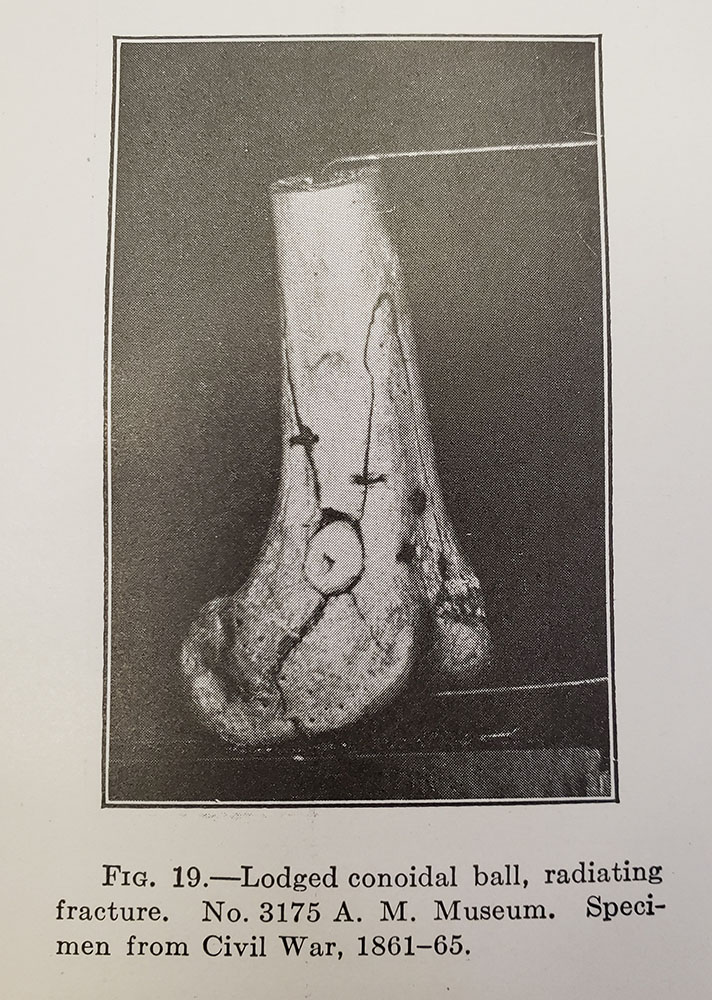
The below image is another example of radiating fractures present in a femur from a lodged conoidal ball.
Before ending this blog post, I really wanted to share a quote by Walter that has resonated with me that I hope may help others see the human skeleton in a different light:
“It is hoped in the following pages to make plain, in some measure at least, that the human skeleton, so often associated unthinkingly with the gruesome symbolism of death, is actually a very wonderful and animated piece of architecture, full of beauty and inspiration for one who looks upon it with a seeing eye and considers its age-long evolution with a comprehending and sympathetic mind.”
Sources:
La Garde, Colonel Louis A. Gunshot Injuries; How they are inflicted, their complications and treatment. NY: W. Wood and Company, 1916.
Truetta, Josep. An Atlas of Traumatic Surgery; Illustrated Histories of Wounds of the Extremities. Oxford: Blackwell, 1949.
Wagstaffe, William Warwick. Student’s Guide to Human Osteology. Philadelphia: Lindsay and Blakiston, 1875.
Walter, Herbert Eugene. The Human Skeleton: An Interpretation. NY: Macmillan, 1918.