– by Wood Institute travel grantee Lindsey Grubbs*
Hysteria posed a unique challenge to the medical profession in the late nineteenth century. As clinicians increasingly relied upon advances in instrumentation and laboratory science to diagnose organic disease, hysteria remained an enigma, mimicking organic disorder without discernable cause. S. Weir Mitchell, notorious for his work with the disorder, understood that what he once called “mysteria” was a condition with “hazy boundaries” that could not responsibly be drawn.[1] But despite this acknowledgement (or perhaps because of it), he spent much of his career attempting to delineate between organic and hysterical disorders.
Earlier this year, I spent two weeks in the Historical Medical Library researching for my dissertation the role of literature in the creation of new psychiatric diagnoses. Seeking evidence of how Mitchell employed narrative techniques as he disseminated his vision of hysteria, I spent most of my time, of course, with the Mitchell collections. His correspondence with other physicians, patients, and literary figures, his case notes, and his lecture notes demonstrated how deeply his diagnostic and literary interests supported one another. While taking a brief Mitchell-hiatus, however, I found a less glamorous set of materials that provided unexpected insight into the solidification of hysterical diagnoses in this period: the clinical notebooks of Charles P. Mercer, a medical student at the University of Pennsylvania. These writings are a fascinating window into just how the diagnostic gaze was trained in Mitchell’s Philadelphia.
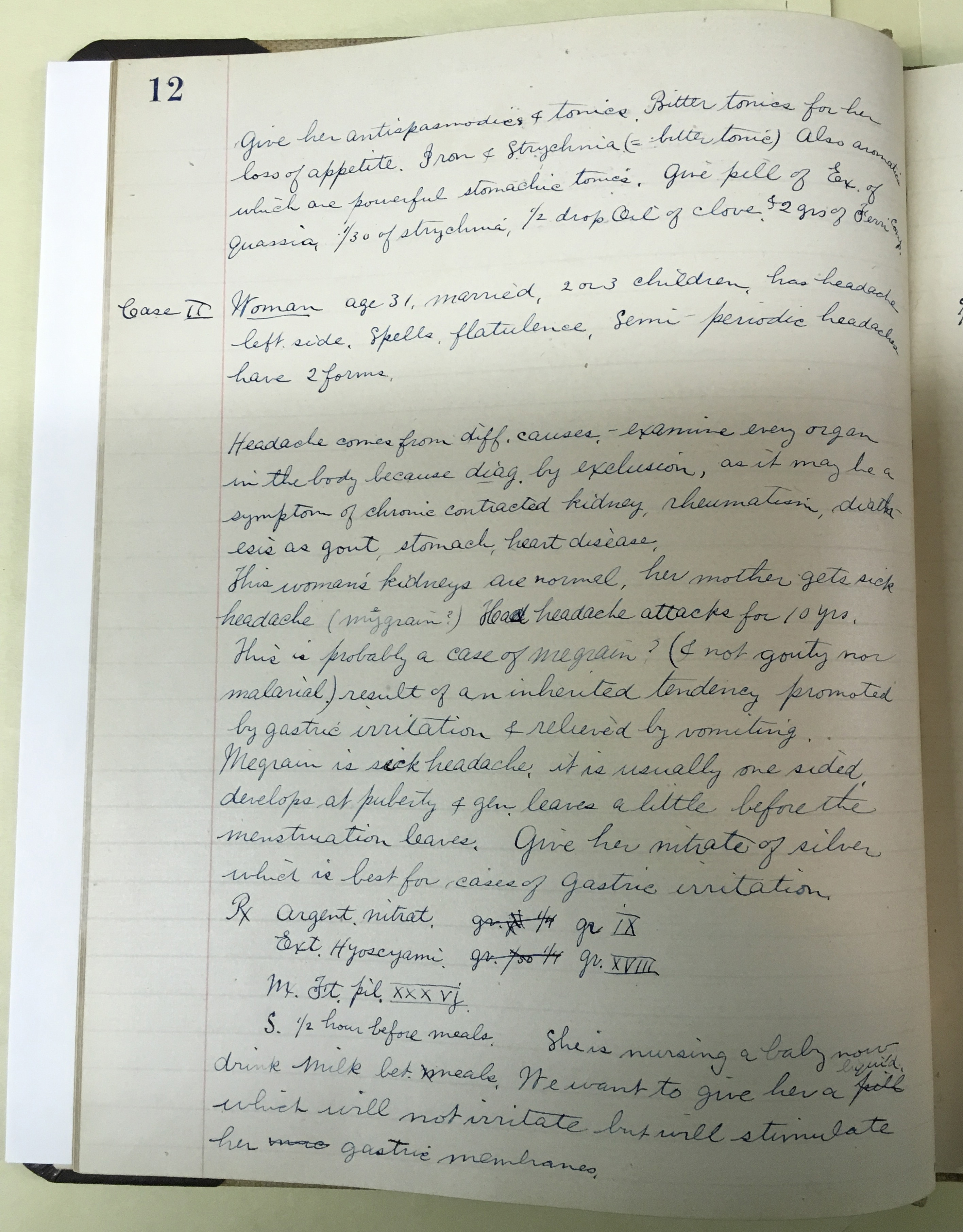
In the typical case, Mercer presents biographical information about the patient, a brief history of the complaint, a step-by-step differential diagnosis with a provisional conclusion, and a treatment plan. Often, a brief didactic interlude will interrupt or precede a case. While published works by established physicians often include extensive case studies, these are retrospectively constructed with a particular claim in mind. They may therefore be the clearest articulation of an individual’s medical philosophy, but their polish obscures the mechanics of the clinical encounter. Mercer’s notebooks, on the other hand, rife with abbreviations and sloppy grammar, appear to be written real-time and reveal the encounter as it unfolds.
Hospital and clinic records often have this same temporal orientation, but, written by practitioners who have internalized the process of differential diagnosis, they lack the explicit communication of the assumptions and norms guiding the process. By showing the scaffolding guiding the construction of a diagnosis in a given case, the notes show how medical philosophies and practices were transferred from one generation to the next, as medical students were trained in patterns of questioning designed to evoke a patient narrative.
Mercer himself does not stand out as a prominent historical figure. Born in Philadelphia in 1864, he graduated with his medical degree in 1891, worked in general practice, and served the Philadelphia Health Department until 1931. His daughter gave the notebooks to Osler-enthusiast Samuel Radbill, because one of them records Mercer’s time in Osler’s clinic from 1887-1889.[2] Radbill wrote about this notebook in 1961 for the Transactions and Studies of the College of Physicians of Philadelphia and donated the materials to the College in 1984.
The collection comprises three notebooks: the first includes 96 pages of notes from nervous disease clinics at the Hospital of the University of Pennsylvania under the direction of Horatio Wood and Francis Dercum from 1887-1889, while the second holds 116 pages of notes on clinics with William Pepper at the same hospital between 1887-1890. The third, from Osler’s clinic, exists only as a typescript, not the original notebook.
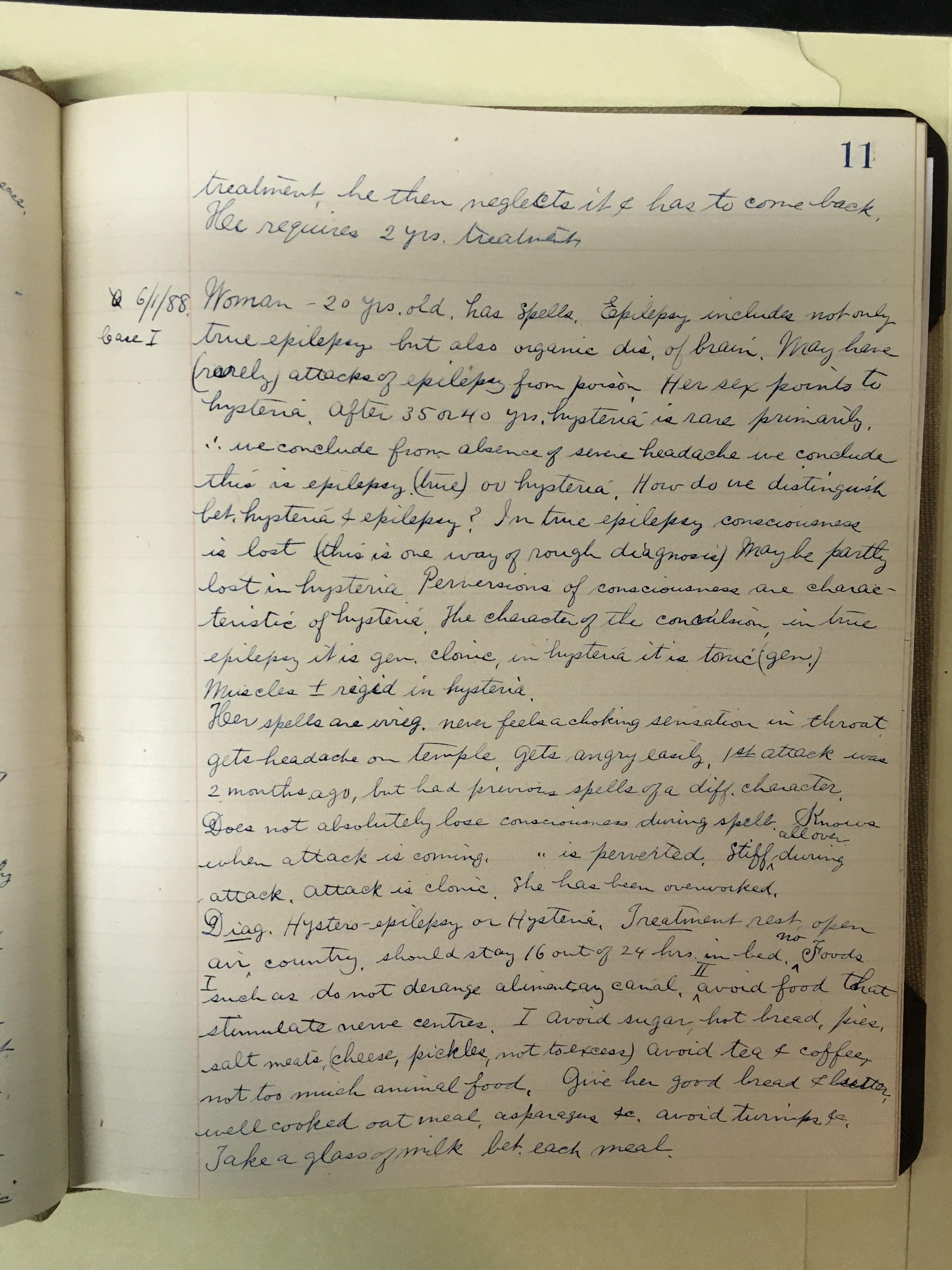
This volume of notes taken in the nervous disease clinics were of particular interest to my project. I give the following case, marked as case #1, 6/1/1888, almost in entirety as an illustration:
Woman – 20 yrs. old, has spells. Epilepsy includes not only true epilepsy but also organic dis. of brain. May have (rarely) attacks of epilepsy from poison. Her sex points to hysteria. After 35 or 40 yrs. hysteria is rare primarily, [therefore] we conclude from absence of severe headache we conclude this is epilepsy (true) or hysteria. How do we distinguish bet. hysteria & epilepsy? In true epilepsy consciousness is lost (this is one way of rough diagnosis) Maybe partly lost in hysteria Perversions of consciousness are characteristic of hysteria. The character of the convulsion, in true epilepsy it is gen. clonic, in hysteria it is tonic (gen). Muscles +- rigid in hysteria.
Her spells are irreg. never feels a choking sensation in throat gets headache on temple. Gets angry easily, 1st attack was 2 months ago, but had previous spells of a diff. character. Does not absolutely lose consciousness during spells. Knows when attack is coming, [consciousness] is perverted. Stiff all over during attack, attack is clonic. She has been overworked. Diag. Hystero-epilepsy or Hysteria. Treatment rest, open air, country, should stay 16 out of 24 hours in bed…. (p. 11).
The frenetic pace of this entry, marked by abbreviations and grammatical errors, shows Mercer speeding to keep up as the case was considered. After giving the briefest introduction, Mercer indicates the possibilities—epilepsy, brain disorder, (maybe) poisoning, and lastly hysteria, which is noted as most likely without to any further examination or questioning simply because of her gender. It is not simply a record of her case, though, and she is used as an opportunity to talk about hysteria in general. For instance, Mercer notes that hysteria is rare after 35, which has no immediate bearing on the case of this woman, and talks in broad terms about how to tell whether a seizure is epileptic or hysteric. After listing general diagnostic facts of the disease, he returns to the patient. Of note, she is diagnosed as hysterical despite having a clonic attack, which is noted as a sign of “true” epilepsy. The assessment, then, is made at least in part on social factors (“Gets angry easily” & “has been overworked”) and on the basis of gender, which influenced their view from the start.
The notebooks suggest how individual cases were used to shape assessments of population-level illness: cases are routinely noted to be “typical” of their type, or used as an example of something atypical, and thus an opportunity to learn about typical expressions. A patient who may seem like an exception that should lead to questioning the validity of diagnostic criteria, then, is used to prove the rule in the inverse.
The constant recurrence of the organic/hysteric question throughout these notebooks highlights neurology’s preoccupation with this question. The hedging “generally,” “maybe,” “rough diagnosis,” reveals the impossibility of making it. In one case, Mercer’s writes: “Rule (practical enough for working purposes) In epilepsy developing inside of 1 year is organic & in 9 out of 10 it is connected with sclerosis of brain or arrest of growth of some convolutions of brain” (p. 9). The test for diagnostic criteria, then, is whether they are good enough for “working purposes”— to get a general sense of tendencies so that steps can be skipped in the diagnostic process, as they were for the woman whose “sex points to hysteria.”
The notebooks obviously cannot serve as a proxy for the diagnostic encounter, which exceeds the linguistic. Of one patient, for instance, Mercer writes, “it has a peculiar look” (9). This “peculiar look,” which cannot be relayed in print, is a reminder of the limitations of written genres. Still, the books provide a blueprint of the architecture of diagnostic pedagogy.
Working with the Historical Medical Library’s extensive student materials provided an important complement to more established ones, and can provide as much insight into the nature and concerns of the medical profession as published works by (in)famous physicians.
Endnotes:
[1] S. Weir Mitchell, “Rest in Nervous Disease: Its Use and Abuse,” in A Series of American Clinical Lectures, Vol. 1, ed. E.C. Seguin (New York, G.P. Putnam’s Sons, 1876), 94.
[2] Samuel X. Radbill, “A Student’s Note Book from William Osler’s Clinics in Philadelphia,” Transactions and Studies of the College of Physicians of Philadelphia ser. 4, vol. 29, no. 2 (October 1961): 77-80.
*Lindsey Grubbs is a Ph.D. candidate in English at Emory University. She received an F.C. Wood Institute Travel Grant from the College of Physicians of Philadelphia in 2017.